
Intraarticular pathology – relevance to hip pain and joint health – Part 1
With ever-increasing resolution of imaging modalities, pathology within the hip joint is easier to identify and locate. There is however, a well-accepted mismatch between pathology and pain, so what is the relevance of hip pathology.
Is all hip pathology irrelevant?
How do we sort out what might be meaningfully associated with pain and relevant to future joint health?
Some pathologic features are common in both symptomatic and painfree populations, while others occur more frequently in those with hip pain. The other consideration is whether structural change may have an impact on joint loading and longer-term joint health. If so, preventative education and exercise strategies may be warranted.
In the next 2 blogs we will explore 4 key pathological changes that are regularly identified in imaging and discuss the possible relevance of hip pathology for pain and joint health.
1. Labral Tear
2. Chondral & Bone Changes
3. Ligamentum Teres Tear
4. Joint Effusion-Synovitis
In today's blog, we will start with the first two topics around relevance of hip pathology - labral tears and chondral and bone changes.
1. Labral Tear
The acetabular labrum does contain nerve fibres for nociception and for proprioception (Alzaharani et al, 2014, Haversath et al 2013), meaning that damage to this structure may contribute to hip joint related pain and also to joint protection. However, a recent systematic review and meta-analysis of the prevalence of labral pathology, revealed that while 62% of those assessed with hip pain had labral tears present on imaging, 54% of those without hip pain also had labral tears (Heerey et al 2018). Therefore, while the labrum may be a source of nociception, presence of labral pathology may be irrelevant to the pain presentation of an individual who presents to your clinic with positive imaging findings.
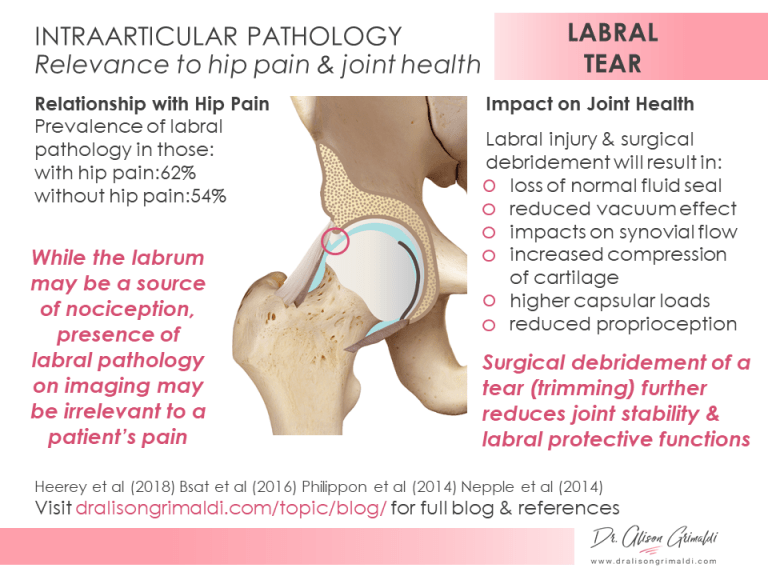
Labral dysfunction is likely to have wider implications beyond pain. The labrum, despite only absorbing 1-2% of weightbearing loads in a hip with normal bony coverage (Henak et al 2011), has some very important functions in joint stability and chondral protection. The labrum deepens the socket and seals the joint, creating an important suction effect with negative intra-articular pressure. This vacuum increases stability and traps fluid between the head of the femur and the acetabulum to assist with cushioning impact loads (Bsat et al 2016). Injury and surgical debridement will result in a loss of the normal fluid seal, reduction of the efficiency of the vacuum, impacts on synovial flow, increased compression of cartilage due to loss of interstitial fluid and higher loads on the capsule. Debridement of the labrum has a significantly greater effect on reducing these joint protection mechanisms than the tear itself, and there is an absence of high-quality evidence for isolated labral debridement (Philippon et al 2014, Nepple et al 2014). Labral reconstruction does at least partially restore these mechanisms and yet, technical difficulty is much higher, availability is not widespread, indications are not clear, and outcomes have again not been well established.
An initial trial of non-surgical load management and exercise strategies with a well-informed physiotherapist is highly recommended for hip pain in the context of an isolated labral tear, prior to consideration of any surgical intervention. Where surgery is warranted, reconstruction would appear to be a superior alternative, when available. A risk-benefit analysis should be discussed with the patient considering a surgical intervention. In particular, a patient must understand that labral debridement does not 'fix' their hip.
2. Chondral & Bone Changes
While there is a much higher prevalence of cartilage defects on imaging in those with hip pain compared with asymptomatic individuals (64% vs 12%) (Heerey et al 2018), cartilage is aneural and therefore not a source of nociception. The relationship between chondral damage and pain is most likely mediated by associated changes in other nociceptive structures such as the adjacent subchondral bone and the capsule with its highly innervated synovial lining.
Bone marrow lesions are much more likely to occur in those with painful hips, and subchondral bone is certainly innervated and may be a source of nociception. Bone marrow lesions are identified on MRI as regions of high signal uptake and therefore higher water content associated with increased bone turnover and increased angiogenesis secondary to bone remodelling processes (Shabestari et al 2016). Subchondral bone changes are usually most evident in regions of cartilage deterioration but may occur prior to the visualisation of cartilage change on imaging. For this reason, it has been suggested that subchondral bone pathology may lead to cartilage degeneration due to alteration of biomechanical force distribution or via release of biomediators that influence cartilage health (Barr et al 2015). Disturbance in the normal homeostasis of subchondral bone results in increased bone turnover, volume and change in stiffness with reduced shock absorbing capacity. If the subchondral bone becomes relatively stiffer, the adjacent cartilage will be forced to absorb more shock, potentially inducing degenerative change in the chondral surface that is unable to adequately attenuate these higher loads (Barr et al 2015).

It is interesting to speculate that ability of the chondral surfaces to absorb load may also influence subchondral bone health. For example, labral pathology and associated impairment of the fluid seal of the central compartment is known to increase cartilage consolidation during loading. If the cartilage, which may still appear normal on imaging, is unable to absorb these increased loads, they will be transmitted to the subchondral bone. Failed bone adaptation may result in redistribution of the loads back to the chondral surface, potentiating the degenerative process. Wherever the process begins, there is evidently an intimate relationship between subchondral bone and the adjacent cartilage with respect to osteochondral load sharing, degenerative change and pain.
As cartilage is avascular, it is reliant on diffusion from subchondral bone vessels and from the synovial fluid, for its nutrition. Interference with either of these sources of nutrition may have adverse effects on chondral health. It has been shown that the primary source of chondral nutrition is from the synovial fluid (Wang et al 2018). If this fluid however contains high levels of inflammatory exudates from the synovium, these may adversely influence cartilage health (discussed in the upcoming blog - Part 2, section 4). Conversely, synovial inflammation (and nociception) may be induced by chondral debris and release of soluble cartilage matrix macromolecules into the synovial fluid, secondary to chondral damage (Atukorala et al 2016).
In summary then, while the labrum is capable of nociceptive signalling, labral pathology is almost as common in those with asymptomatic hips, so the presence of a labral tear on imaging cannot be presumed to be responsible for hip pain. However, a loss of integrity in the labrum does have implications for long term joint health. Surgical debridement does not 'fix the labrum' and restore its function, in fact, it may further reduce its joint protective functions. Closely consider your advice around when/if surgical intervention is required for the painful hip with labral pathology. Chondral pathology and bone marrow lesions are more common in those with hip pain, with health of these tissues and the surrounding synovium intimately related.
In our next blog, we will further examine the relevance of hip pathology, discussing the relationship between ligamentum teres tear, effusion-synovitis, hip pain and joint health.
In the meantime, keep those hips healthy!
References:
- Alzaharani, A., Bali, K., Gudena, R., et al. (2014). The innervation of the human acetabular labrum and hip joint: an anatomic study. BMC Musculoskeletal Disorders, 15(1).
- Atukorala, I, Kwoh, CK., Guermazi, A., et al. (2016). Synovitis in knee osteoarthritis: A precursor of disease? Annals of Rheumatic Diseases, 75, pp.390e5.
- Barr, A., Campbell, T., Hopkinson, D., et al. (2015). A systematic review of the relationship between subchondral bone features, pain and structural pathology in peripheral joint osteoarthritis. Arthritis Research & Therapy, 17:228.
- Bsat et al (2016) The acetabular labrum. The Bone & Joint Journal, 98-B(6):730-735.
- Haversath, M., Hanke, J., Landgraeber, S., et al. (2013). The distribution of nociceptive innervation in the painful hip. The Bone & Joint Journal, 95-B(6), pp.770-776.
- Heerey, J., Kemp, J., Mosler, A., et al. (2018). What is the prevalence of imaging-defined intra-articular hip pathologies in people with and without pain? A systematic review and meta-analysis. British Journal of Sports Medicine, 52(9), pp.581-593.
- Henak CR, Ellis BJ, Harris MD, et al. (2011). Role of the acetabular labrum in load support across the hip joint. Journal of Biomechanics, 44, pp.2201–2206.
- Nepple, J., Philippon, M., Campbell, K., et al. (2014). The hip fluid seal—Part II: The effect of an acetabular labral tear, repair, resection, and reconstruction on hip stability to distraction. Knee Surgery, Sports Traumatology, Arthroscopy, 22(4), pp.730-736.
- Philippon, M., Nepple, J., Campbell, K., et al. (2014). The hip fluid seal—Part I: the effect of an acetabular labral tear, repair, resection, and reconstruction on hip fluid pressurization. Knee Surgery, Sports Traumatology, Arthroscopy, 22(4), pp.722-729.
- Sokolove, J. and Lepus, C. (2013). Role of inflammation in the pathogenesis of osteoarthritis: latest findings and interpretations. Therapeutic Advances in Musculoskeletal Disease, 5(2), pp.77-94.
- Shabestari, M., Vik, J., Reseland, J. and Eriksen, E. (2016). Bone marrow lesions in hip osteoarthritis are characterized by increased bone turnover and enhanced angiogenesis. Osteoarthritis and Cartilage, 24(10), pp.1745-1752.
- Wang, X., Hunter, D., Jin, X. and Ding, C. (2018). The importance of synovial inflammation in osteoarthritis: current evidence from imaging assessments and clinical trials. Osteoarthritis and Cartilage, 26(2), pp.165-174.
Another great Anterior Hip Pain blog

Anterior Hip Pain: Causes & Contributing Factors
Adequate consideration of individual causes and contributing factors is important for best outcomes.

Great Read Allison!
Makes a lot of sense! Especially the loss of seal and loss of synovial fluid with Labral tear or debridement!
Yes, it’s an important consideration. When patients hear the word ‘tear’, they naturally think it needs to be repaired. Most surgeons though are currently doing debridement, rather than repairs, for various reasons. But it is clear that debridement does not restore the function of the labrum and research suggests that it in fact further impairs protective labral functions. So while nociceptive capacity may be reduced, the joint may be at higher risk.