
Total Hip Replacement – Is it time yet?
Guidelines from Dr Patrick Weinrauch, Orthopaedic Surgeon. Includes podcast, infographic & podcast notes. Making the decision to undergo Total Hip Replacement (Total Hip Arthroplasty) is something that patients with hip osteoarthritis (OA) may agonise over - understandably so. Although this is generally a remarkably successful procedure with the potential to substantially improve function and quality of life, it is a big operation with substantial inherent risks and costs. I regularly see patients with hip OA who come to see me with a very specific question in mind - 'Is it time yet? Is it time to get my hip replaced?' There are many considerations that determine when 'the right time for total hip replacement' might be for each individual. In this blog, we have been fortunate to receive some words of wisdom from Dr Patrick Weinrauch, Orthopaedic Surgeon, who generously shared his time and insights during an interview at Brisbane Hip Clinic, in Queensland, Australia. This information will be useful to guide your response when you next see a patient with advanced hip OA.
Listen to the interview here:

Want more? Gain access to the entire video library, all online hip courses, the entire ebook series + exclusive access to pdf resources, live meetings & lots more.
About Associate Professor Patrick Weinrauch :
Associate Professor Patrick Weinrauch is an Orthopaedic Surgeon, founder of Brisbane Hip Clinic in Queensland, Australia. The name of his clinic says it all. He focuses exclusively on the management of hip joint disorders, with a high level of experience and expertise in a full range of surgical procedures for the hip, including hip joint arthroscopy, hip joint preservation surgery, hip resurfacing and hip replacement procedures. Dr Weinrauch is a Fellow of the Royal Australasian College of Surgeons and a Fellow of the Australian Orthopaedic Association, and not only has a busy clinical practice but contributes to education programs for other surgeons and health professionals and to scientific research in this field. Dr Weinrauch has published over 50 peer-reviewed scientific papers and is the Deputy Editor for the International Journal of Advanced Joint Reconstruction. He is currently appointed as an Associate Professor at the Griffith University School of Medicine and has been awarded a Doctorate of Philosophy and Master of Engineering for his research relating to the surgical management of adult hip joint disorders. We are very grateful to Patrick for sharing his valuable time and wisdom.
Podcast Notes
The focus of our discussion was on hip osteoarthritis, a condition suffered by many all around the world. Hip Osteoarthritis is often managed very successfully for a long time with non-surgical care such as that supplied by physiotherapists, but for some, there comes a time when their symptoms and function begin to deteriorate despite their best efforts to look after their hip. Physiotherapists and general practitioners caring for these patients often get asked then, ‘Is it time yet? Is it time for surgery?’
Here, Dr Weinrauch discusses what factors he uses to guide his decision-making process around eligibility for hip replacement surgery
Key points when determining the right time for total hip replacement:
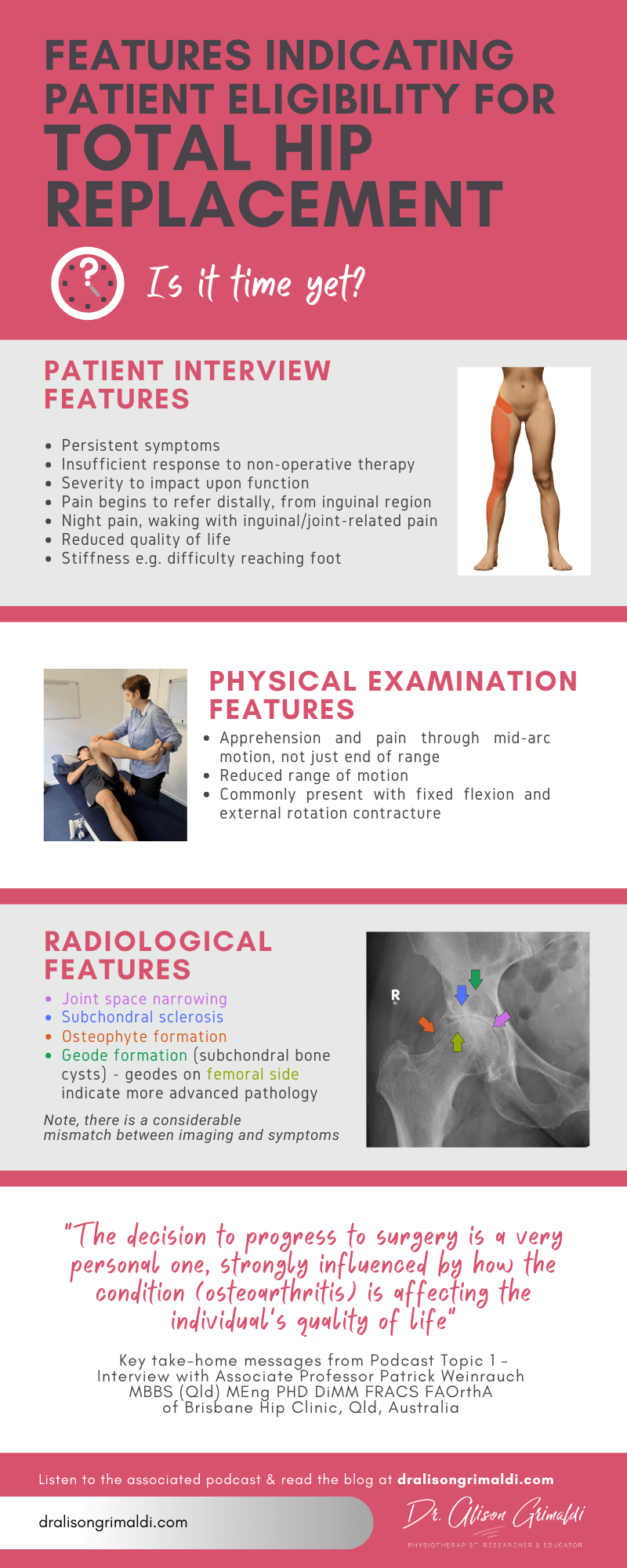
• The decision is very personal one, influenced strongly by how it is affecting the individual’s quality of life
• There is a considerable mismatch between changes on imaging and symptoms, some experiencing only mild symptoms with good function despite advanced osteoarthritis and cartilage loss while others with more focal damage joint may experience quite severe symptoms.
Patient Interview includes:
- Extensive clinical history
- Pain – nature, location, severity
- Function - What can’t you do? What have you had to give up? What would you like to achieve that you can’t because of your hip? If your hip was completely painfree, with no restriction from your hip, how would that change the quality of your life? How would it affect your sporting and recreational pursuits and your family life?
Key criteria for eligibility:
- Severity that is impacting on function
- Persistent pain over a longer duration of time
- Not adequately responsive to non-surgical therapies
- Good trial of non-operative therapies appropriate for their condition
- Established wear on imaging modalities
Adequate previous trial of non-surgical management would typically include:
- Education on hip care and conditioning
- An exercise program for hip specific conditioning
- Injectable therapies
- Oral pharmaceuticals
- Clear indications of patient commitment and compliance to a non-surgical management approach as an initial management strategy
Non-surgical management for osteoarthritic hips works! But there may be limitations with very advanced disease or particular presentations. It must be an appropriate, coordinated program with adequate commitment from patient.
Length of time to persist with non-surgical therapies depends on presentation.
There are two main presentations with hip osteoarthritis:
1. Slowly progressive hip osteoarthritis
- Mild symptoms for many years
- Not particularly intrusive on function initially
- Small modifications in activities over time – “creeps up”
- Use oral medications and therapies intermittently
- Slowly progressive until start to have more meaningful impact on function and quality of life
- A longer trial of non-surgical intervention is appropriate, as they may just be having a flare which will settle again with good management
2. Rapidly progressive hip osteoarthritis
- Subclinical or non-symptomatic advanced osteoarthritis – not aware of having had an underlying hip problem
- At some point develop very severe symptoms, very quickly
- Often a trigger (increase/change activity, slip/fall, heavy impact e.g. missed bottom step), but not always
- In retrospect may recall having some hip stiffness &/or an occasional ‘groin strain
- This group would still have a trial of non-surgical care, but if problems persist, are likely to go to surgery more quickly
Pain location and behaviour associated with hip osteoarthritis
- Most common location is mid-inguinal groin region
- Worse with impact and deep hip flexion
- Labral tears & focal/early chondral lesions more commonly present with localised mid-inguinal or c-sign pain
- Features of advancing osteoarthritis
- Patient begins to experience referred pain to anterior thigh and knee and also anterolateral shin pain is very common, occasionally in the buttock
- Rest pain that is waking the patient. Note, be aware that gluteal tendinopathy may also commonly be associated with night pain, but the region of pain is over the greater trochanter, rather than the mid-inguinal/groin region.
Is hip replacement only recommended for older individuals?
This space has changed considerably
- Prosthetic materials have become more refined
- Bearing surfaces have become much more durable, with high wear-resistance
Therefore, hip replacement has become a more viable option for younger people with severe persistent symptoms and advanced early hip osteoarthritis, after a good trial of non-surgical therapies. This is still a consideration however, for longer life expectancy and therefore greater chances of failure over life span.
Imaging features impacting on the decision around the right time for total hip replacement
Radiographic changes (XRay) associated with hip osteoarthritis
- Joint space narrowing
- Subchondral sclerosis
- Osteophyte formation
- Geode formation (subchondral bone cysts)
- Geodes appear on the acetabular side first
- Presence of geodes in the femoral head indicates later stage pathology & reduced likelihood of a good outcome with non-surgical management
Magnetic Resonance Imaging features of hip osteoarthritis
- Early pathology
- evident first on the acetabular side, in most people
- anterior-superior acetabular rim most common initial region of change
- As pathology advances
- acetabular pathology progresses to encompass a larger area
- then changes develop on the femoral side
- Features that may influence potential effectiveness of joint preserving treatments:
- Degree of hyaline cartilage wear will have a major influence
- Labral pathology relatively less influence on outcome
- dGEMRIC scans
- Not useful in advanced pathology with cartilage loss
- Most useful in earlier stages of pathology to determine the quality of the cartilage, where thickness of the cartilage is relatively normal
- Provides better ability to grade degree of cartilage change than standard MRI, where this can be very difficult
- Not necessary if the patient is a candidate for hip arthroscopy, as arthroscopy provides an opportunity for direct visualisation and palpation of the cartilage surfaces to assess the degree of chondral pathology
That it’s for Part 1 of this interview series. Hope you gained some valuable clinical insights into the right time for total hip replacement. If you are not signed up to the www.dralisongrimaldi.com mailing list, sign up today to ensure you don’t miss the rest of this great series where we’ll be talking about non-surgical options for management of hip OA and a video interview that explores the different prostheses, surgical approaches and their indications. Don’t forget to explore the dralisongrimaldi.com site which contains a wealth of clinically applicable information on all things hip.
Learn more about
CONTEMPORARY DIAGNOSTIC & MANAGEMENT STRATEGIES FOR ANTERIOR HIP & GROIN PAIN, here
Another great Anterior Hip Pain blog

Anterior Hip Pain: Causes & Contributing Factors
Adequate consideration of individual causes and contributing factors is important for best outcomes.
